Healthcare Rankings and the New Geography of Distributed Care

Authored on
Modified
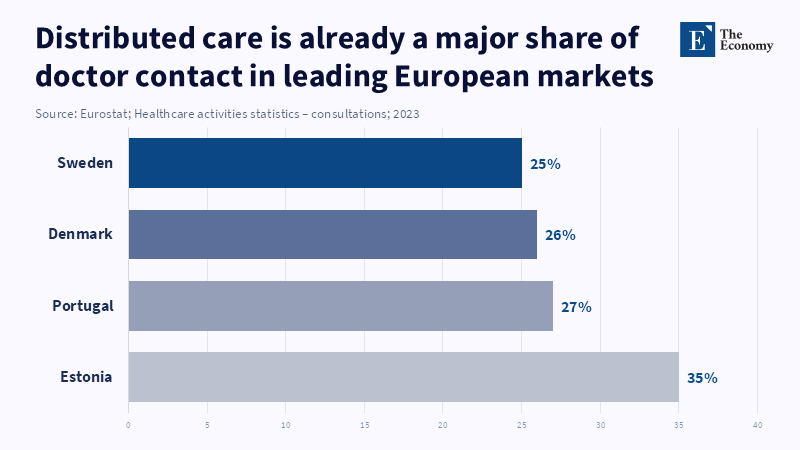
Distributed care is replacing the old healthcare ladder with a more flexible network As care moves across systems, discoverability and interoperability matter more Rankings help patients and buyers navigate a more decentralized market

Healthcare used to be a pyramid. Patients got sick, saw a GP, and if it was more serious, jumped to a bigger hospital, only making it to a specialist setting when the highest level of expertise or technology was needed. It was a formalized, institutional hierarchy. Geography did a lot of that work; Accessibility was the fundamental precursor to who was seen first. Regional institutions could funnel diagnosis and treatment around a select number of sites that were easy to get to. Tertiary centers existed at the top of the pyramid, taking on the most complex patients by way of both clinical and geographic referral processes. That isn't the world we live in anymore. But that pyramid isn't one that entirely applies anymore. It is being disrupted by distributed healthcare systems. Through digitized systems, remote monitoring, telehealth, AI, informed diagnostic tools, and collaborative platforms, care can now be delivered more flexibly across systems, geographies, and severities. That way, patients are less dependent upon being driven along a single local pathway; that way, they can be referred from multiple directions; that way, they can move more freely between providers; that way, they can have access to expert care without climbing that old pyramid. It isn't just treatment that changes; Competition, comparison, observation, and rankings are all different when decentralized healthcare markets are at play.
The old institutional ladder was built on place
In the same market, for generations, it looked like physical space. Local doctors formed your market entry point based on proximity, because most information was then, and even now remains, trapped in paper files, referral relationships, and isolated hospital systems. Hospitals did not win just on volume, but on information: images, consults, lab tests, and inpatient bed availability. And great ones existed atop the ladder, because markets could not always place every specialty, every great piece of equipment, and every intensive care bed across each geography. So stability existed: Patients went up the ladder as the complexity of their illness increased. Competition lived in a range of "market position", their local reach, share of referrals, and size of facility.
This created a clear geography of caring and a clear set of boundaries. Access was defined by where the patient was located, who knew the local doctor, which hospital network possessed the next rung up in the chain, and how fast the networks could communicate with each other. Even where the quality of care was optimal, the system was often short and changed. Expert knowledge was available in the market, but not consistently in time. A second opinion could mean a trip. Oversight might depend upon the presence of the observer. Continuity might depend upon the patient carrying bits of a message about an intermediary. The old ladderbeat, given the physical cost of intimation, i.e., the market was unable to extend expertise widely enough or cheaply enough for it to have any other features.
It is not merely that we now have the technology that has changed; what changed is that this technology now sometimes has the ability to transform the specific architecture of care itself. As health records become more portable, consulting, visiting, and monitoring can all occur away from the hospital walls; the institutional territorial logic is weakened. The patient no longer has to ascend and descend the institutional flight of stairs under the same conditions if information, triage, and clinical oversight can be moved more easily than the patient himself. The line of care now resembles a much more expansive network. That's the basic structural change.
Distributed care turns the ladder into a network
Distributed health systems do not abolish institutions; they alter the pathway of the linkages between institutions. A patient may still go first to a primary care provider, but future encounters are no longer constrained to follow a single local network. The encounter may be remote, in an effort to attract a specialist sooner, or the deterioration may be recorded by a wearable prior to arranging a face-to-face encounter. The digital platform may direct a patient to a diagnostic service in one network, a specialist in another, or, after treatment, a home follow-up model. AI decision support tools can aid triaging, identify patterns in pathology or imaging, and direct routing decisions, at speeds which have hitherto been made manually. Instead of a small provider to a large provider to a higher-tier provider, pathways emerge as a network:
That changes the geographies of healthcare competition quite a bit. Providers are no longer simply competing for the patients that happen to be nearby, or for those that 'drift'in their network by way of traditional referral topographies. They are now competing for visibility and legibility in a more complex and information-intensive marketplace. Discoverability counts seven more now, as patients, employers, insurers, care navigators, and even clinicians have several different ways to 'arrive at a new alternative. Interoperability is increasingly associated with value; Masonelines make that single site that can't easily pass along information a less valuable node in a distributed system of care. Clarity of signals is becoming more important because it's the clinician or patient who can know exactly what the supplying party does best once that supplying party is encountered by way of the distant, new hierarchy.
This is when distributed care makes a market,structure story, rather than a technology story. Telemedicine alone doesn't disperse care; remote monitoring doesn't either. The structural change happens because of the meeting of several digital layers that make it easier to move across providers and settings within a geographically distributed landscape. Patients aren't in one place. You needed to enable the market to get more dynamic, to get more conceptually fluid. And that drove opportunities for specialized providers; new coordinated platforms, new virtual first models, and new institutions to scale up both physical and digital capabilities. But it also created competition for trust because if care becomes freer to move, payers will need new ways to evaluate where to send it.
Why discoverability, interoperability, and signal clarity now matter more
Our old way of doing business set defaults before there was a choice. Geography chose the first provider. The hospital catchment area sets the next. Referral networks provide the specialized markets. Distributed care takes those defaults away. Because care is reachable from anywhere across networks and locations, the market becomes denser for the buyer. There are more choices. More providers compete with each other for attention. More providers enter the choice set. That raises the incentive for discoverability. A provider cannot use distributed care to advantage if referrers, institutional payers, or individual consumers cannot find it, learn about it, and trust it.
Interoperability again becomes an issue for similar reasons. In a distributed system, a provider’s effectiveness is not judged in a vacuum. It is judged in terms of how well it fits into the totality of the care journey. Can it receive useful information fast enough? Can it program outcomes and follow-up info fast enough? Can it plug seamlessly into shared pathways and avoid administrative labyrinths? Distributed healthcare will be inherently inclined to gravitate towards highly plug-and-play, seamless integration with providers. This may sound like a technicality, and it is one, but a technicality is exactly what it is. The provider that is easiest to plug into the patient journey will ultimately be selected repeatedly. Friction ceases to be just an operational inefficiency and becomes a market inefficiency.
Clarity of signal is the third structural challenge. In a dispersed care market, patients and purchasers encounter providers over a domain, not the node of explanation. A specialist clinic makes an appearance at a platform. A virtual service is filed through an insurer. An app suggests a diagnostic provider. A distant monitoring agent joins a chronic care pathway. The purchaser encounters a name, a profile, a claim, an award, a number, perhaps a star rating. And alone, that is not enough. Disaggregated care drives home the advantage of transparent, comparable signals communicating who is credible, who is expert, who is linked, and who is performant in a dense system of care.
The high-performing individuals are not likely to be the loudest. They are likely to be those who make it easier to guess what their function on the care continuum is. They will have established their territory. They will have specified their place within broad pathways. They will have removed the potential ambiguity from the perspective of the patient or institutional buyer. They will have built a conviction that they are capable of providing care across more fractured geographies. In a scattered marketplace, opaqueness will be priced. Transparency is a differentiator.
The rankings function as a navigation device in a decentralized marketplace
What ranks at all in distributed care can actually do. In the old institutional pyramid, everyone used to see rankings as a free extra on top of reputation. They simply topped off a market that was already sorted out by factors like referral psyche and region. Now, more distributed rankings do more than embellish regard: they organize selection. They make possible consumers(kinds of consumers)of careworking patients, cultures, payersto elect the providers, the institutions, to provide care in a marketthat "must be done," face,to,face in the earliest appearance,and is bursting with institutions and modalities. Ranks become a kind of code to a complex system in which the patient could be trafficking across skills, digital interfaces, and institutional spaces and dimensions.
That doesn't mean rankings should necessarily attempt to boil down all of health care into a single list. They shouldn't. But in such a diffuse marketplace, a bit of discipline in the best places only becomes more useful: it can help consumers tease out general hospital skills from specialty expertise, help payers slot digital or venture-backed providers alongside longtime operators, and point interested consumers closer to a credible image, establish sources in niches that didn't exist a decade ago. Good ranking systems can reduce search costs, prioritize individual winners, and help consumers wade through the complexity. They can turn untrustworthy crowdsourced data into something that can be used.
The top list of competing facilities in this environment will not be one size fits all. It will tend to be categorically oriented, will be more transparent, and will mirror the distributed care world more accurately. This means angling toward performance across networks rather than across specific institutions. This means including transparency for agents of care that are strategic players, but not the institutional moms and pops. As health care becomes more malleable, we will need more sophisticated devices to evaluate where the gold standards of care, specialization, and reliability reside.
That's the true strategic importance of distributed care. Not that patients are able to seek advice through the webcam or have diagnostics done there in their living rooms. The key point is that choice spread dependency. The old spread made sense because care moved at the top of that ladder via a tried and true pattern of established dominance. The new spread is equal all over a web of related skills. It's a far more adaptable system, and far harder still to negotiate. That's what makes discoverability more valuable. More providers are competing for time and resources. Interoperability matters more, too. Care pathways don't stay within their comfortable, narrow fields of activity, so the wider the range of barriers they can surmount, the better. The most obvious signs are more valuable still, and rankings can give such signs. They help make a decentralized world more manageable.
Hospitals, specialisms, and local care will all still exist in the future of health care. But the way they exist is changing. Care is becoming less attached to a place and more attached to networks of data, to how services are organized, and bodies of knowledge are shared. This is the fundamental change from the traditional institutional hierarchy to the modern distributed health care domain. In this new domain, the losers are those providers who will not be able to manage across the distributed network channels, thus even subconsciously risking being invisibly unconnectably untrusted to the consumer.
References
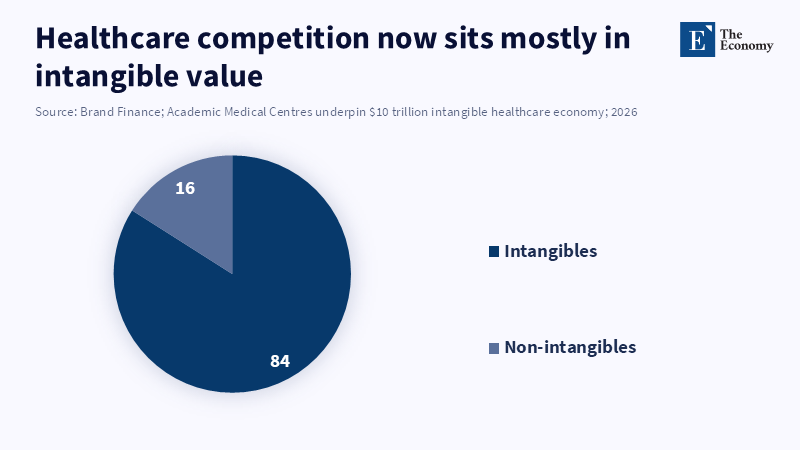
Brand Finance (2026) ‘Academic Medical Centres underpin $10 trillion intangible healthcare economy’. Press release, 5 February.
European Commission (2025) European Health Data Space Regulation (EHDS). Brussels: European Commission.
Eurostat (2026) ‘Healthcare activities statistics – consultations’. Statistics Explained, 10 March. Luxembourg: Publications Office of the European Union.
IQVIA Institute for Human Data Science (2025) Digital Health Trends 2025: Business Models, Evidence Requirements, and Revenue Opportunities. Parsippany, NJ: IQVIA.
Keelara, R., Sutherland, E. and Almyranti, M. (2025) ‘Leading practices for the future of telemedicine: Implementing telemedicine post-pandemic’, OECD Health Working Papers, No. 173. Paris: OECD Publishing. doi:10.1787/496a8ffe-en.
Sehgal, N.K., Guntuku, S.C., Southwick, L., Merchant, R.M. and Agarwal, A.K. (2025) ‘Online reviews of health care facilities’, JAMA Network Open, 8(8), e2524505. doi:10.1001/jamanetworkopen.2025.24505.
Similar Post
















