Healthcare Rankings and the New Economics of Expertise

Authored on
Modified
Size no longer proves expertise in healthcare AI and transparency are weakening the old prestige advantage of big systems Rankings help the market identify real capability instead of inherited reputation

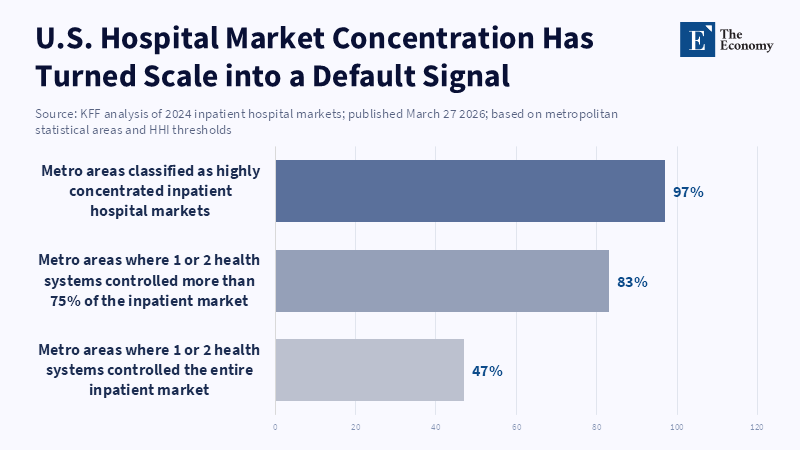
For much of the modern era of healthcare, the market behaved as if institutional size was a proof of clinical quality. Larger campuses, more expansive networks, bigger numbers of specialists, more well-known system brands, all of these signals were interpreted as proof that better medicine was being delivered inside bigger walls. That belief wasn't just cultural; it was ingrained in the market by referral patterns and reimbursement incentives, through advertising, and through decades of healthcare mergers and acquisitions. As of 2024, one or two health systems had a share of the inpatient market in 47% of U.S. metropolitan areas, all metro markets, and 97% of metro markets met the definition of a highly concentrated inpatient hospital market. In that world, size isn't just what draws patients and referrals; it's also what teaches payers and patients how to interpret quality. They come to understand that the bigger the place, the better it is. The trouble with this shortcut is that it's getting less and less trustworthy. The new healthcare competition isn't among the biggest system brands; it's among the systems that can show the most current, relevant, and expert. That's why rankings are now of such value: They allow the market to distinguish star power from substance.
How the system instructed the market to confuse magnitude with knowledge
This was based on valid logic. Larger hospitals commonly had bigger service lines, newer equipment, greater staff pools, and higher referral gravity. They could support high acuity capacity at scale in most service categories. But over time, the market pushed that reality well beyond its reasonable bounds. A statistical indicator that once hinted at likely competence became an industry rule: bigger meant better. The surrounding industry consolidation merely cemented it. KFF data indicated 69% of community hospitals fell under the umbrella of a larger health system in 2023, compared to 58% ten years prior. The ten largest systems already held 22% of all non-federal general acute care hospital beds. And when scale takes on absolute dominancy, the entity itself truly begins to be the evidence. Brand takes the hit. Prestige turns into a marketable value that can be priced.
Hospitals and dominant systems reaped those benefits exponentially. They no longer needed to demonstrate expertise if a buyer just showed up. They could just point to the hospital name, brand, footprint, or building, and that would do most of the marketing. This created a prestige economy on top of the existing care economy, whereby brands could then indicate a sense of premium pricing because the institutional presence mattered in referral streams, patient choice, insurer power, and employer opinion. McKinsey's 2026 consumer research reveals that cost, access, and provisions of credible care really still dominate brand in healthcare, but at the same time reveal a tremendous amount of efforts on the part of organizations to voice features that patients did not necessarily care about. That is, healthcare had monetized that institutional aura for years while the market was rapidly defining the factors that it truly valued behind its back.
And that is the reason why today's debate is often too loosely focused on a trust crisis. Trust is not the beginning of competition. It is a consequence of the repeated demonstration that a provider can solve the problem in front of the buyer. For a long time, large institutions had the luxury of that trust without having to be tested for its since scale was long treated as a proxy for expertise. But when that guidepost decays, trust must be earned in a more vulnerable manner: Expertise, once opaque, becomes transparent, therefore contestable and therefore comparable; the center of gravity shifts: from institutional iconography towards proof.
The demise of the size premium and whether it will reappear
The first crack in the stale model comes when size and price stop correlating to quality. The 2025 GAO report on hospital mergers and acquisitions concluded that hospital and physician consolidation has led to increases in spending and pre-negotiated prices, with, at best, no increases in quality. A 2025 study in JBJS Open, a for-profit open access journal, assessed joint implant pricing: hospital size and system size signaled high commercial prices, while hospital quality and performance did not. That is a market structure issue, not a branding issue. It means large systems have been awarded for their bargaining power and their institutional megastructure, not for digestible results that buyers can make comparisons against. When those become apparent, prestige premiums begin to look less like experimental evidence and more like a market inheritance.
The second crack is technological. The AMA stated in 2025 that 66% of physicians who responded to a 2024 survey were already using AI in practice, up from 38% a year earlier. The FDA's list of AI-enabled medical devices is still growing, offering clinicians and operators an ever more extensive layer of tools for imaging, workflow, triage, and decision support. This is not to say that AI makes hospitals interchangeable, but it does mean that components of expertise that were once bundled within super-sized institutions are becoming more diffuse, more generic, and faster to change. As routine diagnostic support, documentation, navigation, and pattern recognition come into being less of a given above the old prestige hierarchy, the market is less willing to treat sheer size as the best indicator of clinical mastery.
The third crack is transparency. CMS rolled out more hospital price transparency requirements for 2026, with expanded enforcement beginning April 1, 2026. That is important because it no longer forces healthcare purchasers to do battle in a market where cost is for most of them all but off the table until after the fact. Meanwhile, we have normalized online comparison behavior. In April 2026, Pew found that 73% of Americans seek health information from three or more source types, and 22% say they sometimes get health info from AI chatbots. That's not a world in which institutional rep can be assumed to be immune to challenge. It is a world in which buyers navigate, triangulate, and challenge. Old prestige signals are still relevant but no longer monopolize attention.
For what reason is demonstrated competence replacing institutional symbolism
As that shortcut becomes less and less reliable, the industry begins to look for more solid evidence. According to Huron’s 2025 consumer survey, 50% of consumers say great care (including access, skilled providers, and outcomes) is the single most important aspect of their healthcare experience. Similarly, the survey reports 25% are willing to pay a premium for outstanding outcomes and quality, and 24% are planning to switch providers in the next six months, even though 64% say they were satisfied with their most recent care. That's an interesting combination; buyers aren't just asking for trust in the abstract. They're looking for proof that the provider is actually better at doing what they need done. Symbolic assurance is giving way to comparative evidence.
Here is where "the new fight is about trust" runs into its longstanding serious limitations. Trust still counts, but it is no longer chiefly guaranteed through the grandness of institutional scale. Instead, expertise is what bestows trust, since that is what prospective buyers need to see before they are willing to move forward. Huron found performance on reputation for "trustworthiness, reliability and quality" remains a factor in audience switching, but "new and innovative treatments," efficiency, affordability and access to schedules ranked just as highly. A McKinsey 2026 survey hits the same point from a different angle: in particular, 60% of surveyed Americans felt they were overpaying, while unmet expectations about the cost of care remained "the most common source of dissatisfaction." Only providers who can render their competence transparent are being well rewarded.
And that change is speeding up, because the knowledge is now spreading faster. The new techniques, devices,supported workflows, AI, and aided operating models are not staying locked in the biggest institutions for much time. Smaller, specialist hospitals, centers of excellence, and high-performance service lines can stand a better chance of making a case for excellence now than they could ten years ago, as long as they can prove why. The simple question is no longer, "How big is this system?" It's, "Who's best at this decision, this procedure, this pathway, this result, right now?" The marketplace is getting more precise, more category-centric, and less forgiving of mere prestige without evidence. That's not the death of trust. It's the rebirth of trust in evidence.
When rankings of hospitals become much more useful
In that world, rankings don't hover just beyond the boundary of the market, serving as decoration in the media, but instead serve as a comparative approach to manage a costly type of uncertainty. The real alternative to rankings isn't perfect information; it is a noisy collection of names of referrals, advertising, gossip, celebrity, fragmentary information and institutional memory. And that collection of things has always favored big systems: they are the name brands that are easiest to remember and denigrate. Rankings matter because they impose a more ordered comparison. They help buyers to ask a more complicated question than "who is the biggest." They encourage asking who performs well in a specialty, who is up and coming, who can consistently produce depth, and who has the most obvious expertise. In markets with high levels of asymmetries of information, that role is infrastructure.
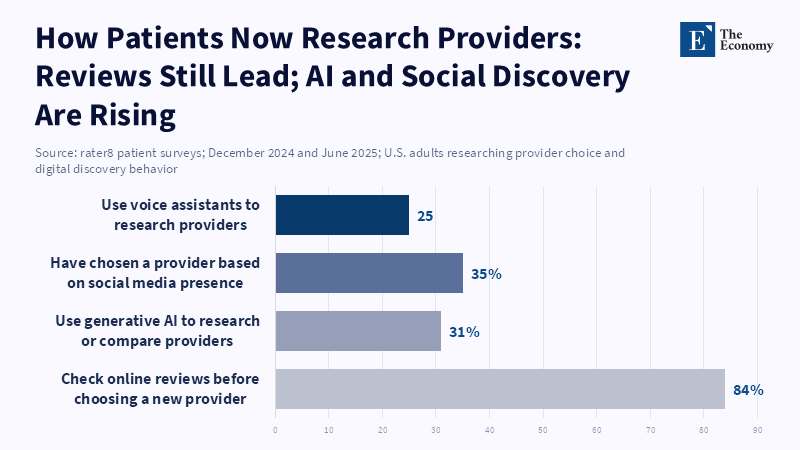
The tangible case is easy to observe in behavior. Huron found that reference from healthcare professionals still mattered most when consumers picked a new provider, but online reviews and rankings had grown close behind traditional references and the provider's web presence in decisions. Rater8 reported in 2025 that 84% of patients look up online reviews before picking a new provider, and 31% use generative AI tools like ChatGPT or Google AI Overviews to research or compare providers.41 Once the discovery layer is digital, every provider is being judged in a competitive market, whether it wants to be or not. Rankings help structure that market. They produce a defensible abbreviation that does not give excessive weight to just visibility or leave buyers stranded in a bog of fragmented claims.
The usual objection is that rankings may simply oversimplify quality, or that they reward visibility over value. That risk is very real if rankings are badly constructed. But when the market already reads the old prestige order as indicative of quality (and allows that to swamp consensus), silent praise protects incumbency rather than fairness. The better course is not to avoid rankings altogether, but to develop more effective comparison tools: smaller schools, transparent metrics, more recent information, and more refined granularity between size, reputation, and true competence. That is especially crucial now, for the decline of size as a mark of deposit of institutional wisdom leaves the market with less information, not more. Rankings are not worthless because they distort, but rather because they are not based on enough information. They are valuable because they help us purge inherited prestige and establish credible standards of performance. With AI, transparency, and more timely information, that is, again, a vital part of how the market reeducates itself to identify excellence.
References
American Medical Association (2025) ‘AMA: Physician enthusiasm grows for health care AI’. 12 February.
Centers for Medicare & Medicaid Services (2026) ‘Hospital Price Transparency’. 23 March.
Cordina, J., Buchter, J., Bochtler, E. and Lee, M. (2026) ‘Healing consumer confidence through AI-powered, human-centered healthcare’. McKinsey & Company, 19 February.
Government Accountability Office (2025) Health Care Consolidation: Published Estimates of the Extent and Effects of Physician Consolidation. GAO-25-107450. Washington, DC: U.S. Government Accountability Office.
Harris, A.B., Wang, J., Lugo, E., Wang, Y., Bai, G. and Jain, A. (2025) ‘Size, Not Hospital Quality and Performance, Influences Commercial Prices’. JBJS Open Access, 10(4). doi: 10.2106/JBJS.OA.25.00258.
Huron Consulting Group (2025) Unlock Patient Loyalty: New Healthcare Consumer Insights.
Pasquini, G., Stocking, G., Kikuchi, E., Pula, I. and Yam, E. (2026) ‘Where Do Americans Get Health Information, and What Do They Trust?’ Pew Research Center, 7 April.
Similar Post
















